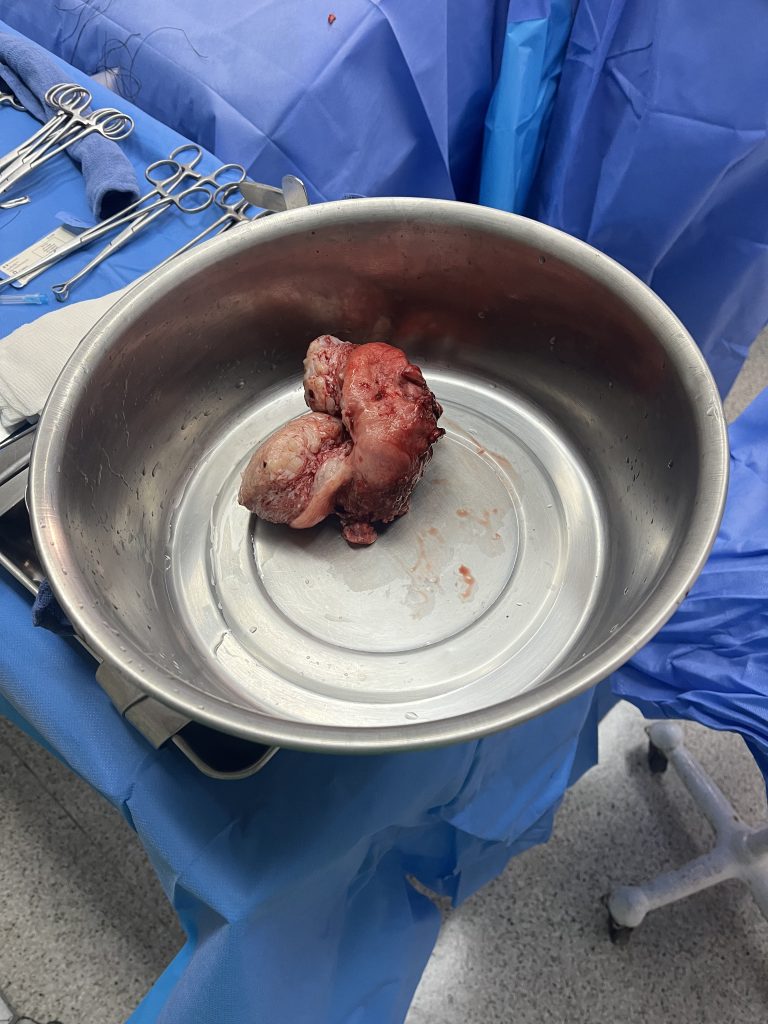
Warning: This blog contains a graphic image of surgery
Hello Everyone!
This week Sam and I moved around various units. We were supposed to be in ICU, but Monday-Wednesday there were no patients. Monday we continued to work on our case study presentation. Then, Tuesday and Wednesday, we observed in the OR. Some notable surgeries that we watched were a total thyroidectomy and an excision of a submandibular gland. A total thyroidectomy is when the surgeon takes out the patient’s whole thyroid gland. This surgery is very interesting to watch in the beginning but it gets tedious because the surgeon has to cauterize and tie off veins since excessive blood in the neck could be damaging to the patient’s airway. Excision of a submandibular gland is a common surgical procedure to remove one or both of the salivary glands under the jaw. This patient specifically got their gland removed because they had a blockage in their duct.
On Thursday, we got to see a total hysterectomy which was fascinating to watch. A total hysterectomy is when the uterus, ovaries, cervix, and fallopian tubes are removed. We got to look up close and dissect the organs afterward which was very interesting. It was surprising to see how small the uterus was, it was about the size of a fist before it was cut open. One of the previous weeks in the OR we saw a dilation and curettage which is a procedure to remove tissue from inside your uterus. So it was fascinating to see the inside of the uterus and make the connection of where someone would remove tissue for this diagnostic test. The surgeon also showed us the cervix, and it was crazy to see how small the cervix and its opening are on a non-pregnant woman because it is hard to imagine it can open up to accommodate a fetus during childbirth.
On Friday, Sam and I were in the ICU. We started the morning learning about all the medication in a “crash cart”, and working on medication calculations. Then, we were each given our patient to monitor, take vitals, feed, bathe, turn, and any other care they would need. My patient required vitals to be taken every hour, strict NPO, and urine output monitored every hour. My patient had a Glasgow Coma Scale of 15 which is super high, and abnormal for a patient in ICU. The GCS assesses a person based on their ability to perform eye movements, speak, and move their body. These three behaviors make up the three elements of the scale: eye, verbal, and motor. A person’s GCS score can range from 3 (completely unresponsive) to 15 (responsive).
After our duty on Friday Sam and I made a trek to the Manila Airport to go to Palawan! Palawan is a popular beach island in the Philippines. We got in late Friday night. So, Saturday morning we woke up bright and early to seize the whole day in El Nido, Palawan. We met up with ALL of the IWU Phillipine interns and went on an island-hopping tour. The tour was amazing, we got to explore 5 small islands, go snorkeling over coral reefs, and kayak in the Big Lagoon. The Big Lagoon is a famous body of water with caves you can explore and swim in.



Sunday, Sam and I headed back to the airport to trek back to Santo Thomas.
Thank you for reading! Talk to you next week!